 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Tanzania Journal of Health Research, Vol. 12, No. 1, January, 2010 SHORT COMMUNICATIONS Role of microscopic examination of stool specimens in the diagnosis of campylobacter infection from children with acute diarrhoea in Kampala, Uganda S.E. MSHANA1,3*, M.L. JOLOBA1, A. KAKOOZA2 and D. KADDU-MULINDWA1 1Department of Medical Microbiology, Makerere
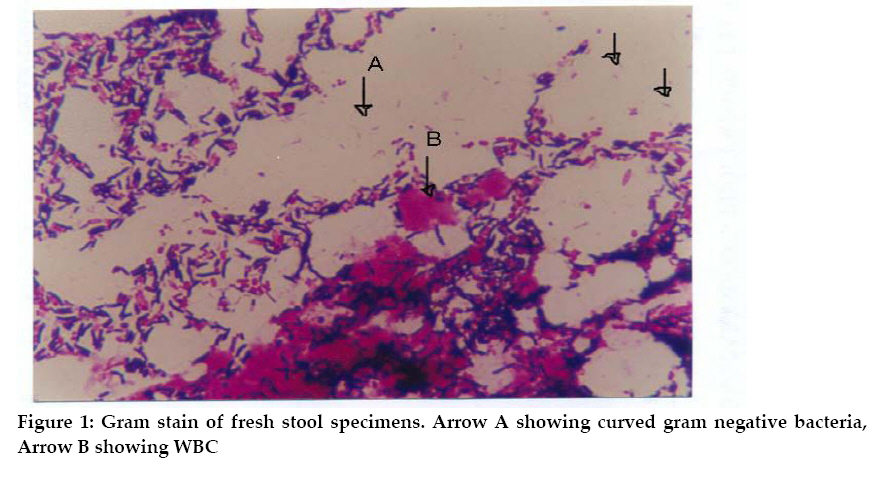
University Medical School, Kampala, Uganda * Correspondence: Dr. Steven E. Mshana; E-mail: mshana72@yahoo.com Received 2 December 2009 Code Number: th10012 Abstract Campylobacter species are a frequent cause of enteritis and less often of extraintestinal infections in humans. The diagnosis of campylobacter infection depends mainly on culture which is difficult and expensive to be done as routine in most clinical microbiology laboratories in the developing countries. This study was conducted to determine the sensitivity and specificity of Gram-stain of the stool in diagnosis of campylobacter infection, using culture as the gold standard. A total of 226 stool specimens were obtained from children with acute diarrhoea, attending Mulago Hospital in Kampala, Uganda. Stool smears were made and conventional Gram stain done using 0.3% carbol-fuschin as counter stain for 5 minutes. Mucous part of the stool was cultured in Charcoal Ceferaperazone Deoxycholate Agar and blood contained selective media. A total of 21 stool samples (9.3%) were positive by culture and 17 (7.5%) by Gram stain. Sensitivity and specificity of Gram stain in the diagnosis of campylobacter infection was 76% and 99.5%, respectively with positive predictive value of 94.1%. A total of 127 (56.2%) had white blood cells (WBC) in stool and there was strong association between WBC in stool and the presence of campylobacter infection (P=0.001). Gram stain is a good alternative in diagnosis of campylobacter infection in place where facilities for culture are limited. Key words: Gram stain, sensitivity, specificity, Campylobacter, Uganda Campylobacter is a genus in the family campylobactericea. The genus has 18 species of which five have been associated with diseases in man. These include Campylobacter jejuni, C. fetus, C. lari, C. coli and C. upsaliensis (Tauxe et al., 1988). In developing countries where bacterial culture is not routinely done infection rate has been found to be up to 35% (Taylor, 1992). The isolation of these organisms is expensive and most of clinical microbiology laboratories in the developing countries do not perform routine culture for these organisms (Elmer et al., 1998). Diagnosis of Campylobacter infection mainly depends on culture of stool specimens using selective media such as Skirrow, Charcoal Ceferaperazone Deoxycholate Agar (CCDA), and Modified Preston Agar. Culture of these organisms is expensive and difficult in developing countries where campylobacter infection is prevalent. Campylobacters can be visualized with Gram stain using 0.3% basic fuschin as counter stain. In few studies conducted Gram stain examination of the stool specimens has sensitivity of 66%-94% and specificity above 95% (Murray et al., 1995; Taylor et al., 1993). Simultaneously examination of faecal white blood cells (WBC) is possible during Gram stain; WBC has been reported in as few as 25% to as many as 80% of culture proven cases of campylobacter infection (Taylor et al., 1993). This study was carried out to evaluate the role of microscopic examination of the stool specimens in the diagnosis of campylobacter infection among children with acute diarrhoea using culture as gold standard at Mulago Hospital in Kampala, Uganda. This cross-sectional study involved a total of 226 stool specimens. Stool specimens were obtained serially from children with acute diarrhoea, attending Mulago Hospital in Kampala Uganda for a period of 4 months from July to October 2005. Stool specimens were collected using wide mouth screw cap containers (HIMedia laboratories Pvt Limited, Mumbai, India). All specimens were transported to the laboratory and analyzed within 2 hours of collection. The slide smear of the fresh stool was made on new slide; it was air dried and heat fixed. The Gram stain was done using conventional gram stain procedures with 0.3% Carbol-fuschin (Sigma-Aldrich) as counter stain for five minutes (Sazie & Titus, 1982). Mucous part of the stool was inoculated on blood free charcoal based selective media (CCDA) and blood contained media selective for campylobacter (BioMerieux, Paris, France). The incubation was for 48hrs under microaerophillic environment generated using gas pack and anaerobic jar 150 system (BioMerieux, Paris, France). A known Campylobacter spp from Medical research council Entebbe was used as control during incubation. Suspected colonies were further identified using catalase, oxidase, and susceptibility to nalidixic acid, cephalothin and Hippurate hydrolysis (Murray et al., 1995; Lindblom et al., 1995). All slides were examined by two individuals independently under light microscope using X10 objective for WBC and X100 oil immersion objective for campylobacter bacteria (Figure 1) before culture results were known. Results were entered in the laboratory book and computer using SPSS 10 software. Sensitivity, specificity and positive predictive value of Gram stain in the diagnosis of campylobacter infection were calculated as shown in Table 1. Fisher exact test was done to establish the association between WBC and campylobacter infection. Among 226 specimens analyzed 21 (9.3%) were positive by culture for campylobacter infection (Table 1). Using culture as gold standard the sensitivity and specificity of Gram stain of fresh stool specimens in the diagnosis of campylobacter infection was 76% and 99.4%, respectively. Similar high sensitivity and specificity have been reported in other studies (Murray et al., 1995). Use of 0.3% Carbol-fuschin as counter stain in Gram stain for longer duration increases the sensitivity in demonstrating the shape of Campylobacter. Relatively low sensitivity (<44%) has been observed using safranin as counter stain (Ho et al., 1982). Patients usually shade up to 106-109 of these organisms per gram of stool, making microscopy examination of the stool easy. Gram stain can be positive when the shading is as low as 103 organisms per gram of the stool (Steele & McDermott, 1984). Table 1: Gram stain in relation to culture of Campylobacter spp among children with acute diarrhoea
Sensitivity: TP/TP+FN= 16/21, 76%; Specificity: TN/TN+FP=204/205, 99.5%; Positive predictive value: TP/TP+FP=16/17, 94%; Negative predictive value: TN/TN+FN=204/209, 97% One sample was smear positive and negative culture. This is likely to be due to previous use of antibiotics or poor survival of these organisms on bench. This sample was traced to the patient who didn’t use any antibiotic so the poor survival could explain this different. It may also be considered as false positive due to microscopic error examination (Wang & Murdoch, 2004). Five samples which were smear negative but positive culture were considered as false negative. This could be explained by low shading of these organisms due to use of antibiotics or late stage of the infections. Three of these samples were from children with onset of diarrhoea of 7, 8, 13 days (mean onset = 4 days). The low shading due to late stages of infection is likely to have contributed to the false smear negative of the samples (Wang & Murdoch, 2004). No explanation was found for the other 2 samples. Table 2: Association between presence of WBC in stool and culture for Campylobacter spp
WBC can be a good predictor of campylobacter infection. WBC were found in 19 (90.4%) of proven culture positive stool specimens (Table 2). The difference in isolation rate between stool specimens with WBC and those without was significant P=0.001 (Murray et al., 1995). Most studies concluded that only stool specimens with WBC should be cultured for campylobacter. The presence of WBC in stool specimen is due to invasive nature of Campylobacter jejuni in the pathogenesis of enteritis (Wang & Murdoch, 2004). Culture is the golden standard in the diagnosis of campylobacter infection. However, culture is expensive, takes long duration, and culture plate can have high contamination rate of faecal normal flora making reading of plates difficult and time consuming. Gram stains although less sensitive when compared to culture can be used in the diagnosis of campylobacter infection in poor-resource countries where facilities for culture are limited. This method can provide results within 30 minutes of receiving specimens. Also microscopy examination of stool samples for WBC can be used as predictor of campylobacter infection; this is due to strong association between the two. A large study which includes control group is recommended to evaluate and standardize the role of microscopic examination of stool in the diagnosis of Campylobacter infection. Acknowledgements We thank the staff of Microbiology Department Makerere Medical School and Paediatric Department Mulago Hospital for their cooperation. This work was supported by the grant from WBUCHS to SEM References
Copyright 2010 - Tanzania Journal of Health Research The following images related to this document are available:Photo images[th10012f1.jpg] | ||||||||||||||||||||||||||||||||||||||||||||
| |||||||||

{kind=link}